Ovulation Induction: What It Is, How It Works, And Who Benefits Most

A calendar marks the days of the menstrual cycle, with a pregnancy test placed across the fertile window, capturing the idea of tracking ovulation and fertility.
If your periods are irregular, infrequent, or absent, and particularly if you have been diagnosed with PCOS, there is a good chance that ovulation is not happening regularly. And without ovulation, natural conception is not possible. Ovulation induction is a fertility treatment that uses medication to stimulate the ovaries to develop and release an egg. It is the first step in the fertility treatment pathway for women with ovulatory disorders, and for many women — particularly those with PCOS — it is the only step needed.
It is simpler, less invasive, and less expensive than IUI or IVF. It works by stimulating the body's own reproductive process rather than replacing it. And in appropriately selected women, it is highly effective.
Dr. Shachi Singh, consultant gynaecologist and infertility specialist at Prakash Hospital, Sector 33, Noida, explains exactly how ovulation induction works, how monitoring is done, which medications are used, what the success rates look like, and how to know when to move to the next step.
Who Needs Ovulation Induction?
Ovulation induction is specifically for women who are not ovulating reliably or not ovulating at all. The relevant conditions include:
PCOS (Polycystic Ovary Syndrome): The most common indication. PCOS disrupts the hormonal signals that drive ovulation. Many women with PCOS do not ovulate every cycle or do not ovulate at all. Ovulation induction restores this process.
Hypothalamic dysfunction: The hypothalamus — the brain region that controls the hormonal cascade for ovulation — can be suppressed by excessive exercise, significant caloric restriction, very low body weight, or severe psychological stress. The result is absent or very infrequent periods. Ovulation induction can stimulate ovulation when hypothalamic suppression is the cause.
Unexplained infertility: In women with regular cycles who have been unable to conceive after 12 months of trying, stimulated ovulation induction combined with IUI can improve pregnancy rates above what timed intercourse alone achieves — even when a specific ovulatory disorder has not been identified.
Ovulation induction is NOT the right treatment if:
- Both fallopian tubes are blocked (sperm cannot reach the egg)
- Male factor is severe (not enough functional sperm)
- The primary problem is structural — fibroids distorting the uterine cavity, significant uterine septum, etc.
These situations require different treatment approaches, and using ovulation induction without addressing them wastes time.
The Medications: Letrozole and Clomiphene
Two oral medications are used for ovulation induction. They work differently, but both stimulate follicle development.
1. Letrozole (Femara) — The Current First-Line Choice
Letrozole is an aromatase inhibitor — a drug that blocks the conversion of androgens to oestrogen. At low doses used for ovulation induction, this temporary oestrogen reduction causes the pituitary gland to produce more FSH (follicle-stimulating hormone), which drives follicle development in the ovary.
Why has letrozole become the preferred first-line medication:
- A landmark clinical trial by the NICHD Reproductive Medicine Network — the largest ever conducted in PCOS ovulation induction — demonstrated that letrozole produces significantly higher live birth rates than clomiphene in women with PCOS
- Lower multiple pregnancy rate (predominantly singles rather than twins)
- No significant anti-oestrogenic effect on the uterine lining or cervical mucus (an issue with clomiphene — see below)
- Generally well-tolerated with fewer side effects
How it is taken: Days 3 to 7 of the menstrual cycle (or days 5 to 9 in some protocols). Taken orally once daily for 5 days. Standard starting dose is 2.5 mg; can be increased to 5 mg or 7.5 mg if the initial dose does not produce adequate follicle development.
2. Clomiphene (Clomid) — The Older, Established Alternative
Clomiphene works by blocking oestrogen receptors in the brain (at the hypothalamus and pituitary), causing the body to perceive low oestrogen levels and increase FSH production. Widely used since the 1960s and still an appropriate choice in many situations.
Limitation: Clomiphene's anti-oestrogenic effect — which is how it stimulates FSH — also reduces the quality of cervical mucus (making it harder for sperm to penetrate) and can thin the uterine lining (reducing implantation). These effects are less pronounced with letrozole, which is one reason letrozole has superseded it as first-line in PCOS.
How it is taken: Days 3 to 7 or 5 to 9. Standard dose: 50 mg daily for 5 days. Dose can be increased to 100 mg or 150 mg if no response at lower doses.
3. Injectable Gonadotropins
When oral medications fail to produce adequate follicle development (in medication-resistant PCOS or hypothalamic dysfunction), injectable FSH preparations can be used. These directly stimulate the ovaries without going through the pituitary pathway. They are more potent and require careful monitoring to avoid over-stimulation (multiple follicles developing simultaneously, increasing the risk of multiple pregnancy). Typically used in conjunction with IUI rather than timed intercourse alone when needed.
Monitoring — How the Cycle Is Tracked
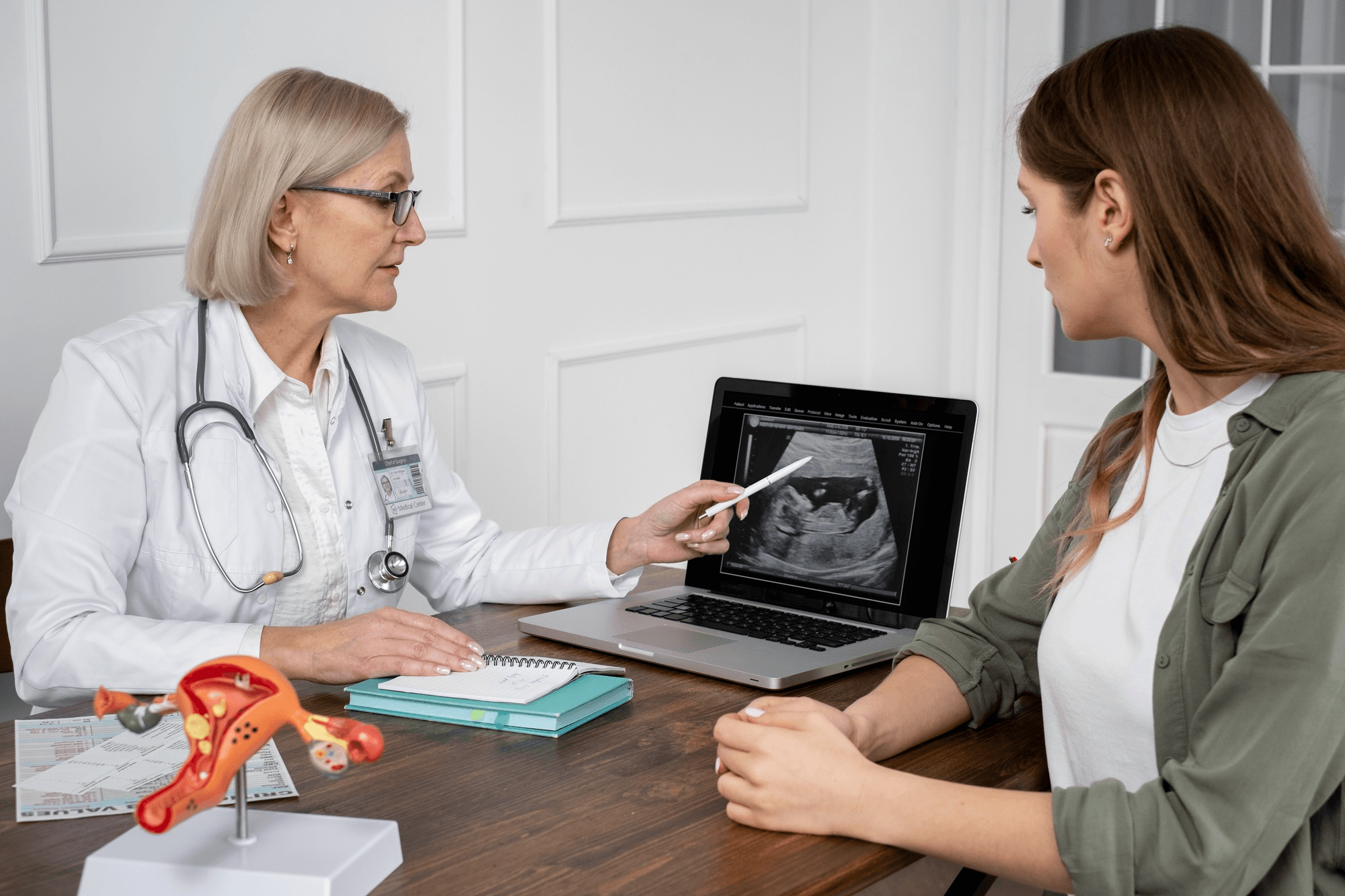
A woman talks to a gynecologist as they review an ultrasound report, emphasizing the importance of getting checked if periods stop or become irregular.
Ovulation induction is not taken and then waited on blindly. The response of the ovaries to the medication needs to be tracked for two reasons:
- To confirm that an adequate response is occurring (at least one follicle developing to the right size)
- To time intercourse or IUI correctly — or to identify over-response (too many follicles) and cancel the cycle
Monitoring involves transvaginal ultrasound — typically done on day 2 to 3 (baseline, before medication starts), then again around day 10 to 12 after the medication course, and further if needed.
What the ultrasound looks for:
- Number of developing follicles
- Size of follicles (ovulation typically occurs when the dominant follicle reaches 18 to 22 mm)
- Uterine lining thickness (should be at least 7 to 8 mm at the time of expected ovulation)
When a follicle reaches the target size, ovulation can be triggered with an injection of hCG (human chorionic gonadotropin) — which mimics the natural LH surge that triggers ovulation. This allows precise timing of intercourse or IUI.
If monitoring shows too many follicles (typically more than 3 to 4 above 14 mm): The cycle may be cancelled — the couple is advised to avoid intercourse — to prevent the risk of high-order multiple pregnancy. This situation is more common with injectable gonadotropins than with oral letrozole or clomiphene.
Success Rates — What to Expect
Ovulation rate with letrozole in PCOS: Approximately 60 to 70% per cycle at standard doses.
Pregnancy rate per cycle: Approximately 15 to 20% per ovulatory cycle — comparable to the per-cycle conception rate of normally fertile couples.
Cumulative pregnancy rate after 3 cycles: Approximately 40 to 50% in women who ovulate in response to medication.
After 4 to 6 cycles without conception: Even when ovulation is achieved in every cycle, conception rates drop in subsequent cycles. Most fertility specialists reassess the treatment approach after 4 to 6 ovulatory cycles without pregnancy — either moving to IUI (if not already combined) or to IVF.
Ovulation Induction Combined with IUI
Ovulation induction and IUI are frequently used together — particularly in unexplained infertility and mild male factor infertility.
The combination gives the fertility process two boosts simultaneously:
- Ovulation is confirmed and timed precisely
- The best sperm are concentrated and deposited at the ideal location
Success rates with combined ovulation induction + IUI are higher than either alone.
Side Effects and Risks
Clomiphene: Hot flashes, mood changes, headaches, blurred vision (unusual — report immediately if this occurs). The risk of a twin pregnancy is approximately 5 to 8%.
Letrozole: Generally well-tolerated. Occasional joint aches, fatigue, and hot flashes. Significantly lower multiple pregnancy rate than clomiphene.
Ovarian hyperstimulation syndrome (OHSS): The ovaries over-respond to stimulation, becoming enlarged and producing excess fluid. With oral letrozole and clomiphene at standard doses, severe OHSS is rare. It is more of a concern with injectable gonadotropins, particularly in women with PCOS who have naturally high follicle counts. Monitoring specifically aims to detect early signs of over-response. Mild OHSS (bloating, mild pelvic discomfort) is manageable at home. Severe OHSS (significant abdominal distension, difficulty breathing, rapid weight gain) requires medical attention.
Multiple pregnancy: The primary risk of ovulation induction, particularly at higher doses or with injectable gonadotropins. Twins are manageable but carry significantly higher risks than a singleton pregnancy. Higher-order multiples (triplets or more) are associated with serious maternal and neonatal risks and are specifically what monitoring aims to prevent.
Ovulation Induction and Fertility Care in Noida and Greater Noida
A woman holds an ovulation test kit, applying a sample, showing the step of checking fertile days during the menstrual cycle.
Dr. Shachi Singh at Prakash Hospital, Sector 33, Noida, provides ovulation induction as part of a comprehensive fertility treatment pathway for women across Noida and Greater Noida — including baseline evaluation, stimulation protocol, ultrasound monitoring, trigger injection timing, and coordination with IUI when appropriate.
If you have irregular or absent periods and are trying to conceive, a proper evaluation — including hormonal blood tests and baseline ultrasound — is the starting point.
To book a consultation with Dr. Shachi Singh, call: +91 97023 46853
Clinic Hours: Monday to Saturday, 9 AM – 6 PM | Sunday, 10 AM – 2 PM
Clinic Address: D-12A, 12B, Sector-33, G.B. Nagar, Noida, Uttar Pradesh 201301
Frequently Asked Questions
What is the difference between letrozole and clomiphene for ovulation induction?
Both stimulate follicle development. Letrozole is now preferred as first-line in PCOS because clinical trials show it produces higher live birth rates and lower multiple pregnancy rates. Clomiphene's anti-oestrogenic effect on cervical mucus and uterine lining is a disadvantage that letrozole does not share.
How many cycles of ovulation induction should I do?
Most fertility specialists recommend 3 to 6 cycles of monitored ovulation induction before reassessing. After 3 ovulatory cycles without conception, combining with IUI or moving to IVF is typically considered. After 4 to 6 total cycles without success, the plan should be reviewed.
Can I take letrozole or clomiphene without monitoring?
Technically, but it is not recommended. Monitoring confirms whether ovulation is occurring, times intercourse or IUI correctly, and — critically — identifies over-response before high-order multiples are conceived. Unmonitored cycles are less effective and carry unnecessary risk.
Is ovulation induction the same as IVF?
No. Ovulation induction stimulates the ovaries to produce one or a small number of eggs that are released naturally — fertilisation occurs inside the body. IVF retrieves multiple eggs from the ovaries, fertilises them in a laboratory, and places embryos back into the uterus. Ovulation induction is far simpler, less invasive, and less expensive than IVF.
Can ovulation induction cause twins?
Yes — slightly higher twin rate than natural conception, particularly with clomiphene. Letrozole has a lower multiple pregnancy rate. Monitoring aims to prevent high-order multiples by cancelling cycles where too many follicles develop.
This blog is written for educational and informational purposes only. Please consult Dr. Shachi Singh or a qualified infertility specialist for an evaluation and treatment plan specific to your situation.


